From MDLinx, by John Murphy
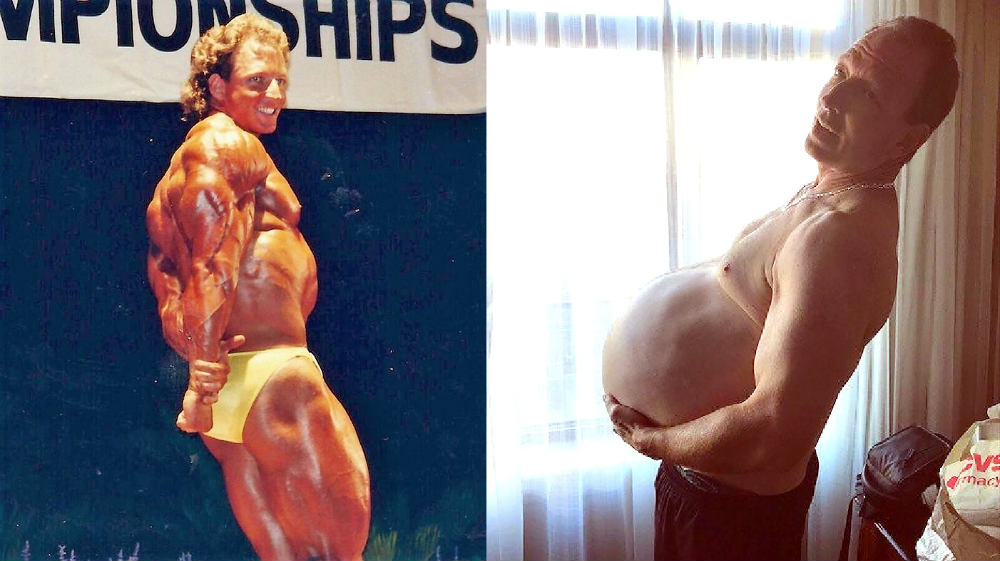
The progression of this hereditary disease was slow but relentless. More and more cysts grew in Gene’s kidneys. As the organs filled with fluid, they become larger and larger.
The average kidney is supposed to be the size of your fist, but Gene’s kidneys were each larger than a football—possibly the largest kidneys ever recorded.
“We’re not quite sure how big because I can’t do a full scan properly with dye,” Gene said. “But the guess is that they’re over 10 pounds each or more.”
The larger his kidneys got, the worse they functioned. But Gene didn’t want to end up on dialysis like his father. He decided to seek a kidney transplant. Someone suggested that he go see transplant surgeon Mikel Prieto, MD, at the Mayo Clinic in Rochester, MN.
What eventually followed was a marathon 12-hour surgical procedure in which Dr. Prieto removed both of Gene’s massive diseased kidneys, then implanted a healthy kidney from a living donor.
The surgery withdrew at least 19 liters of fluid from Gene's body, and he weighed 50 pounds less after the procedure.
Watch this compelling video from the Mayo Clinic to see the extent of Gene’s disease as well as the complicated surgical procedure that followed, and also who stepped up to the plate to donate a kidney after Gene’s unique recruitment efforts to locate a donor.
Dialysis & Politics
From Healio, Nephrology News & Issues, A Viewpoint
Restricting third-party payments discriminates against patients on dialysis
Kidney disease has a frightening way of leveling the playing field – rich, poor, black or white, no one plans for the eventuality of losing the function of an essential organ. Although we know certain demographic groups are affected more frequently than others, for the most part, CKD and kidney failure are scarily indiscriminate with universal impact. When the kidneys go, no matter the size of one’s bank account, the options are the same if active therapy is the chosen route: a transplant or life-sustaining dialysis care.
Although CKD and ESRD do not discriminate, large U.S. insurers are working hard to create a double standard – one that allows wealthy patients who can pay out-of-pocket the right to obtain private health insurance, while prohibiting less affluent individuals from doing the same. It is an effort that undermines patients’ fundamental right of choice and creates a new pre-existing condition exclusion: being poor.
Although there are not a great number of choices when it comes to treating kidney failure, since the creation of Medicare’s ESRD benefit in 1972, Americans have been afforded options when it comes to their insurance coverage. For some, Medicare is the best option; but for others, maintaining private insurance through their employer, COBRA or an individual plan is ideal. Private insurance often provides better, more robust coverage than government programs. Some patients have family members who also require coverage – making it logical to retain one private plan, rather than duplicate cost-sharing requirements across different plans. In nearly half of the states, patients who qualify for Medicare because of ESRD may not be able to access Medigap plans and, therefore, wish to rely upon private insurance, which may have more favorable cost-sharing obligations or expanded coverage. Out-of-pocket costs are high even with Medicare coverage and often run more than $7,000 per year; if patients with ESRD and their family members have separate coverage, this number can be more than double.
Regardless of the reason, historically, patients with kidney failure have been given the right to choose what works best for them and their families, but only for a limited duration of up to 30 months under the Medicare Secondary Payer (MSP) statute.
The option for private insurance coverage has always been there, but if some insurers have their way, it will only be available for the wealthy. The MSP statute already restricts this right and caps the duration for which any health plan must provide for coverage. No matter how long these patients have paid for private health care insurance, they cannot keep it. They must transition to Medicare for primary coverage. This results in a substantial taxpayer subsidy for the insurance plan. Yet they want to push as many patients as possible onto government coverage as soon as possible.
From PR News Wire
Highlights Dialysis Industry's Rip-off of Consumers, Patients
Supporters of California's Prop. 8 ballot initiative launched television ads across the state this week highlighting dialysis corporations' rip-off of consumers and patients with kidney failure.
"One-hundred fifty thousand dollars a year – that's how much big dialysis corporations charge some patients each year – a 350 percent markup above the cost of care," says the ad's narrator, dialysis nurse Megallan Handford of Corona, Calif."Dialysis corporations are making a killing – driving up insurance rates while patients report bloodstains and cockroaches in their clinics."
Supporters are spending $11.3 million to air the 30-second spot on 33 channels throughout the San Francisco Bay Area, Los Angeles, Sacramento and San Diego.
Opponents of Prop. 8 have committed $72.7 million to defeat the initiative, according to campaign finance reports. The total comes entirely from dialysis companies and is led by the industry's two largest corporations, DaVita and Fresenius, which contributed $40.8 million and $23.1 million, respectively.
"No matter how much the opposition spends to scare the public, I know how bad the clinics are and I'm hopeful California voters will see through the smoke and hold dialysis corporations accountable," said Tangi Foster, a 10-year dialysis patient from Los Angeles, who appears in the ad. "If the dialysis companies truly cared about their patients, they would have spent all that money on improving patient care rather than trying to buy off voters."
Prop. 8 limits dialysis corporations' revenues to 15 percent above the amount they spend on patient care and pushes them to invest more in hiring additional staff, buying new equipment, and improving facilities. The California Legislative Analyst's Office estimates 80,000 Californians with life-threatening kidney failure get treatment in dialysis clinics.
DaVita and Fresenius made a combined $4 billion in profits from their U.S. dialysis operations in 2017, and the profit margin of their clinics is nearly five times higher than an average hospital in California. The two companies own and operate 72 percent of all dialysis clinics in the state.
People with kidney failure often must undergo dialysis treatment three days a week at clinics to remove their blood, clean it, and put it back in their bodies. Each treatment lasts three to four hours.
To see the more than 130 organizations supporting Prop. 8, visit www.yeson8.com.
PKD Research
Biomedical engineers at USC have been awarded a $2.4 million federal grant to study how nanoparticles can treat kidney disease, the university announced Oct. 2.
The National Institutes of Health has conferred its New Innovator Award of $2,433,330 to Eun Ji Chung, an assistant professor of biomedical engineering at the USC Michelson Center for Convergence Bioscience.
Chung will apply the NIH innovation grant – one of only four ever given to USC – to advance research at the junction of biology and nanotechnology.
She aims to study how a nanoparticle can ferry various types of medicine to treat autosomal dominant polycystic kidney disease, an inherited disorder difficult to treat with dialysis or a kidney transplant. The trick: How sneak a targeted drug into a kidney and prevent it from being eliminated by the body.
“Our approach is the first of its kind and represents a paradigm shift from current therapies to treat polycystic kidney disease,” Chung said in a statement.
Chung and others to have received New Innovator Awards will be recognized at an NIH High-Risk, High Reward Research Symposium in June 2019.
Health business reporter Dana Bartholomew can be reached at dbartholomew@labusinessjournal.com. Follow him on Twitter @_DanaBart.
This is to inform the general public that Kidney donors are needed from all blood groups by Manipal Hospital, each donor gets ($550,000.00USD). Advance payment will be paid first to the donor before the operation will commence after which the balance will be paid after the completion of the operation. hurry now and contact us Via Email:(manipalhospitalofficial@gmail.com), WHATSAPP NUMBER : +18573099679
ReplyDeleteBest regard : Dr Aritra Ghosh.